Toxoplasma gondii
01 Life Cycle
Toxoplasma gondii belongs to the genus Toxoplasma, family Sarcocystidae, order Eucoccidiorida. It is also known as Toxoplasma gondii (Nicolle & Manceaux).
It is a crescent-shaped protozoan that can invade the central nervous system of humans. As an intracellular parasite, it circulates with the blood, reaches all parts of the body, and damages the brain, heart, and ocular fundus, leading to weakened immunity and various diseases in humans.
Its life cycle requires two hosts:
- Intermediate hosts: reptiles, fish, insects, birds, mammals, including canines and other domestic animals.
- Definitive hosts: felines (members of the cat family).
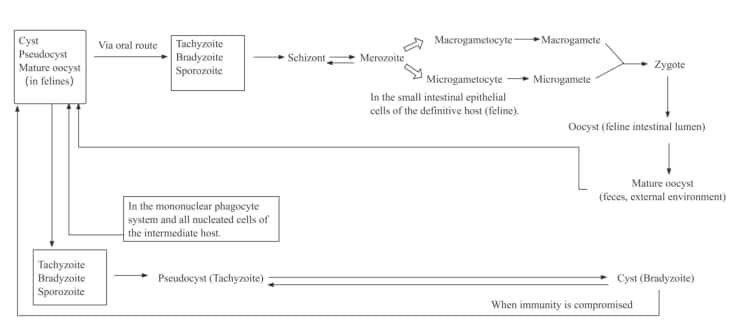
Toxoplasma gondii has a complex and diverse life cycle, which is mainly divided into five stages:
1. Tachyzoite Stage
Tachyzoites replicate asexually within nucleated cells of intermediate hosts (including felines, humans, and other mammals). When numerous parasites fill the entire host cell cytoplasm, they form a pseudocyst.
2. Bradyzoite Stage
Under specific conditions, tachyzoites transform into bradyzoites, which are enclosed by a resilient cyst wall to form tissue cysts. Bradyzoites proliferate continuously inside the cysts, can re-invade new cells under certain circumstances, and persist long-term within host tissues.
3. Schizont Stage
Bradyzoites or sporozoites undergo schizogony within the intestinal villus epithelial cells of felines, forming aggregates of merozoites known as schizonts.
4. Gametocyte Stage
Merozoites invade other intestinal epithelial cells and develop into gametocytes, which further differentiate into male (microgametocytes) and female (macrogametocytes) gametocytes. Male and female gametes fuse to form a zygote, which eventually matures into an oocyst.
5. Sporozoite Stage
Sporogony occurs inside the oocyst, resulting in the formation of two sporocysts; each sporocyst then differentiates into four sporozoites, completing the full life cycle of the parasite.
02 Epidemiology
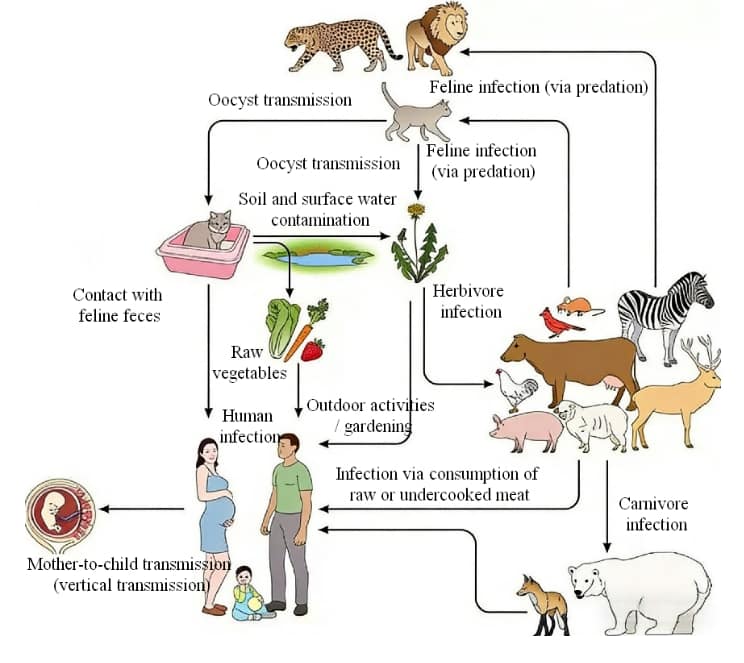
1. Sources of Infection
Felines, other mammals, and birds serve as reservoir hosts for Toxoplasma gondii, with felines as the primary source. Animals carrying tissue cysts are also infectious. Infected pregnant women act as a direct source of infection for their fetuses.
2. Routes of Transmission:
Congenital Infection:Infected pregnant women transmit the parasite to fetuses transplacentally. During maternal parasitemia, the protozoan can also contaminate amniotic fluid and cause intrauterine infection via the fetal gastrointestinal tract.
Acquired Infection:The fecal-oral route is the main transmission mode. Felines and other definitive hosts shed large numbers of oocysts in feces; these oocysts contaminate food, water, or environments and infect new hosts via the digestive tract. Transmission also occurs via contact with infected canines, felines, or their feces without hand hygiene, as well as through sexual contact, blood transfusions, organ transplants, damaged skin/mucosa, or respiratory droplets.
3. Population Susceptibility
The general population is universally susceptible to Toxoplasma gondii infection, with higher rates among animal breeders, slaughterhouse workers, and medical staff. Individuals with severe illnesses (malignant tumors, lymphogranuloma), long-term immunosuppressant users, and immunocompromised patients (e.g., AIDS) are highly vulnerable to clinical toxoplasmosis.
4. Epidemiological Characteristics
Toxoplasma gondii has a global distribution, with most cases being latent asymptomatic infections. In China, the infection rate ranges from 0.28% to 47.3%, higher in rural areas than cities and in adults than children. High-risk occupations include animal breeders, slaughterhouse workers, meat/fur processors, and veterinarians.
03 Hazards and Clinical Symptoms
Pets:
Toxoplasma gondii infection in pets mainly presents as acute and chronic symptoms.Chronic symptoms mainly include anemia, anorexia, lethargy, recurrent diarrhea, ocular symptoms such as iritis, and a small number of cases develop neurological symptoms like paralysis.Acute symptoms mainly include high fever, anorexia, dyspnea with cough, vomiting and diarrhea, sometimes hemorrhagic diarrhea. Pregnant pets may suffer from abortion. A small number of felines may develop complications such as pneumonia or ocular infection.
Humans:
Toxoplasma gondii infection is mainly transmitted via the digestive tract, with symptoms ranging from mild to severe.Primary infection may resemble influenza or meningitis, with symptoms including fever, headache and muscle pain.For immunocompromised people, such as pregnant women, the elderly or those with immunodeficiency diseases, toxoplasma infection can cause severe health problems including retinitis, encephalitis, myocarditis, and even death.Toxoplasma infection in pregnant women may also lead to serious consequences such as abortion, premature birth and neonatal malformation.
Note: Pathogenesis of Toxoplasma gondii in Humans
After invasion, Toxoplasma gondii enters the bloodstream via regional lymph nodes or directly, causing parasitemia. No specific immunity exists in early infection; parasites spread rapidly to organs and proliferate intracellularly as tachyzoites until host cells rupture. Released tachyzoites reinvade adjacent cells, causing focal tissue necrosis and acute inflammation dominated by mononuclear cell infiltration.
In chronic infection, parasitemic dissemination only occurs when cysts rupture and host immunity is impaired. The parasite can target any organ, with predilection for the brain, eyes, lymph nodes, heart, lungs, liver and muscles. Once specific immunity develops, circulating parasites are cleared, and tissue cysts form (most commonly in the brain and eyes) for long-term latent infection.
When host immunity drops, ruptured cysts release bradyzoites that trigger tissue necrosis and immediate hypersensitivity reactions with severe granulomatous inflammation.
Lymph nodes are the most commonly affected site in acquired toxoplasmosis, with characteristic follicular hyperplasia and macrophage aggregation, no typical granulomas.
Ocular lesions feature necrotic foci with inflammatory cell infiltration, starting with necrotizing retinitis and progressing to choroiditis, iridocyclitis, cataract and glaucoma.
Cerebral injury presents as meningoencephalitis with necrosis and microglial nodules; congenital cases involve periventricular calcifications, vascular inflammation and hydrocephalus.
Lung lesions show white nodules and necrotic plaques; the spleen is enlarged and necrotic with perivascular infiltration.
04 Pathogen Diagnosis
1. Serological Testing
Serological testing determines infection by detecting Toxoplasma gondii antibodies in pet serum, including IgM and IgG, which indicate recent infection and previous infection respectively.
2. Colloidal Gold Immunochromatography
Commonly known as test strips, this method is easy to operate and time-saving, but has relatively low sensitivity and is prone to interference, resulting in large result errors. Thus, it can only be used for preliminary screening.
3. Direct Smear Method
Operation: Collect pet blood or tissue fluid for direct smearing, stain with Giemsa stain, and observe under a microscope. The detection of Toxoplasma gondii trophozoites or cysts indicates infection. This method has a low detection rate and requires high operator skills.
4. PCR Testing
PCR testing confirms infection by amplifying Toxoplasma gondii DNA fragments, with extremely high sensitivity and specificity. It can accurately diagnose infection in pets without interference from other pathogens, and supports multiplex detection of multiple pathogens. It is currently widely recognized and adopted in the industry.
05 Treatment Recommendations
Treatment of toxoplasma infection should be individualized based on the pet’s condition. Sulfonamides are the first-choice drugs for toxoplasmosis.
Acute Stage Treatment: Alternate oral administration of pyrimethamine, sulfadiazine, spiramycin and other drugs.
Central Nervous System Infection: Pregnant women and patients with visceral toxoplasmosis are mainly treated with oral spiramycin; pyrimethamine and sulfadiazine may also be used alternately.
Immune Supportive Therapy: Immunocompromised patients may receive immune enhancers as adjuvant treatment.
Other Supportive Treatments: Antibiotics may be used to prevent infectious complications.
Closely monitor the pet’s symptoms during treatment. If any discomfort or worsening occurs, seek veterinary care promptly. After treatment, follow the veterinarian’s instructions for re-examination, usually including blood tests to confirm clearance of Toxoplasma and evaluate efficacy.
Chronic Stage Treatment: Use specific anti-Toxoplasma drugs combined with immune enhancers. Note that broad-spectrum anthelmintics cannot eliminate Toxoplasma.
06 Prevention measures
The key to preventing toxoplasma infection lies in blocking transmission routes and improving immunity:
Dietary Adjustment: Avoid eating undercooked meat and food potentially contaminated with Toxoplasma.
Avoid Direct Contact with Pet Feces: Wear gloves when handling pet feces and wash hands thoroughly afterward. Keep the pet’s living environment clean, and regularly clean litter boxes and other materials that may contain Toxoplasma oocysts.
Proper Exercise: Boost immunity in both pets and humans to reduce infection risk.
Regular Physical Examinations: Pets should receive regular Toxoplasma PCR testing at veterinary hospitals. If a pet is diagnosed with toxoplasmosis, pet owners, especially pregnant women, should undergo Toxoplasma testing at a hospital.