Comprehensive Analysis of Clostridioides difficile Infection in Pets | Watch Out for Post-Antibiotic Diarrhea, Toxins A and B Cause Severe Harm
Comprehensive Analysis of Clostridioides difficile Infection in Pets | Watch Out for Post-Antibiotic Diarrhea, Toxins A and B Cause Severe Harm
Gastrointestinal symptoms worsening after antibiotic use in pets are most likely associated with Clostridioides difficile infection. Clostridioides difficile is a Gram-positive anaerobic spore-forming bacillus widespread in the natural environment and the intestinal tracts of pets. The bacterium itself has low pathogenicity; however, Toxin A (enterotoxin) and Toxin B (cytotoxin) it secretes are the primary culprits triggering intestinal inflammation and damage in pets. Its spores feature extremely strong resistance, facilitating transmission in veterinary clinics and multi-pet households. As a zoonotic pathogen, it requires heightened vigilance. Friendly reminder: this article is quite lengthy, kindly ask all veterinary practitioners to read it thoroughly.
I. Core Characteristics
Clostridioides difficile belongs to the genus Clostridium and is an obligate anaerobe. Its hallmark traits are highly resistant spores and toxin-mediated pathogenicity, which distinguish it fundamentally from other enteric bacteria such as Campylobacter coli and Yersinia enterocolitica. Its key properties are listed below:
Morphology and Classification
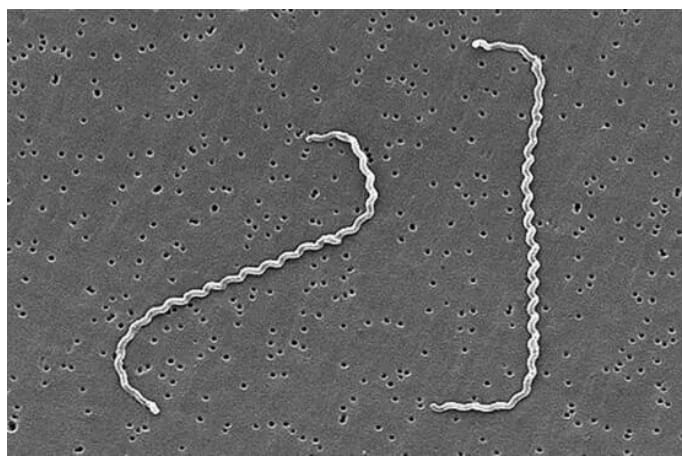
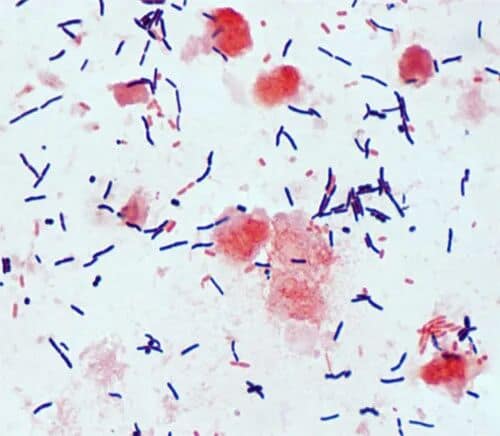
It is a Gram-positive anaerobic spore-forming bacillus with variable rod or fusiform shapes and blunt rounded ends. It lacks capsules but possesses flagella for motility. Oval spores develop at the terminal or subterminal position of bacterial cells, drastically boosting its resistance after sporulation, which constitutes a major challenge for clinical prevention and control.
Physicochemical Properties (Key for Disinfection)
It is an obligate anaerobe that cannot multiply under aerobic conditions; only its spores can survive. It can colonize long-term in anaerobic niches including pet intestines, soil and feces. The spores exhibit exceptional resistance: they survive months to years under normal temperature and dry conditions, and 6–12 months in feces. They are insensitive to routine disinfectants such as alcohol and quaternary ammonium salts, and only susceptible to chlorine-based disinfectants (diluted 1:100), peracetic acid and high temperatures (boiling at 100°C for 10 minutes, autoclaving). Naturally resistant to multiple antibiotics (penicillins, cephalosporins, quinolones, tetracyclines, etc.), it is only susceptible to a limited number of antibiotics including metronidazole, vancomycin and fidaxomicin — this is the core reason why antibiotic overuse readily triggers infection.
Colonization Characteristics
It has a broad host range and colonizes the intestines of dogs, cats, pigs, humans and other species. The subcarriage rate in healthy dogs and cats is approximately 3%–10%. The carriage rate can rise to 20%–40% in multi-pet households, hospitalized pets in veterinary clinics, and pets receiving long-term antibiotic therapy. After spores enter the intestinal tract, the bacteria act merely as transient non-pathogenic organisms if the gut flora remains balanced; they rapidly proliferate and produce toxins once dysbiosis occurs.
Key Pathogenic Mechanism
Clostridioides difficile itself is non-invasive, and its pathogenicity fully relies on two secreted exotoxins: Toxin A (enterotoxin, TcdA) and Toxin B (cytotoxin, TcdB). Most virulent strains produce both toxins simultaneously; a small subset only produces Toxin B with milder pathogenicity, while non-toxigenic strains lack pathogenic capacity entirely.
II. Core Virulence Factors: Toxin A and Toxin B
Toxin A and Toxin B are the primary culprits behind Clostridioides difficile infection. Though structurally similar, they differ greatly in target sites, pathogenic effects and clinical significance. Distinguishing them accurately helps assess disease severity and implement scientific treatment plans.
(I) Toxin A (Enterotoxin, TcdA)
As the major enterotoxin secreted by Clostridioides difficile, Toxin A is a high-molecular-weight protein toxin with a molecular weight of approximately 308 kDa. Its primary functions are destroying the intestinal mucosal barrier and triggering abnormal intestinal secretion, directly resulting in diarrhea, abdominal pain and other symptoms. Its specific properties are as follows:
- Target sites: It mainly binds to glycoprotein receptors on the surface of small intestinal and colonic epithelial cells in dogs and cats. It attaches specifically to mucosal cells without penetrating them, exerting effects only on cell surfaces and mucosal layers.
- Pathogenic mechanism: It disrupts intercellular tight junctions and increases the permeability of the intestinal mucosal barrier. It stimulates mucosal cells to secrete massive amounts of water and electrolytes, raising intestinal osmotic pressure and causing watery diarrhea. Meanwhile, it induces inflammatory factors in the intestinal mucosa, aggravating mucosal congestion, edema and exudation.
- Clinical manifestations: Symptoms are localized mainly in the intestines, including watery diarrhea, mild abdominal pain (arched back and tenesmus in dogs and cats), and mucoid stool. Symptoms are relatively mild, and severe cases rarely occur with Toxin A alone. Combined with Toxin B, it significantly exacerbates mucosal damage.
- Other properties: It is relatively heat-labile and can be inactivated by heating at 60°C for 10 minutes. It can be degraded by trace proteases in the intestinal tract with weak toxicity, and its clinical detection rate is lower than that of Toxin B.
(II) Toxin B (Cytotoxin, TcdB)
Toxin B is a potent cytotoxic protein secreted by Clostridioides difficile, with a molecular weight of roughly 270 kDa. It directly damages intestinal epithelial cells and induces cellular necrosis. Its toxicity is 10–100 times that of Toxin A, making it the key factor responsible for severe infections such as pseudomembranous enteritis. Its detailed characteristics are listed below:
- Target sites: It targets intracellular Rho-family GTPases in intestinal epithelial cells, penetrating cells to directly destroy cytoskeleton integrity.
- Pathogenic mechanism: It modifies Rho proteins, leading to cytoskeleton disorder, cell apoptosis and necrosis, as well as superficial ulceration. It provokes severe inflammatory responses, forming “pseudomembranes” composed of fibrin, necrotic cells and inflammatory cells on the mucosal surface — the hallmark of pseudomembranous enteritis. In severe cases, it enters the bloodstream through damaged mucosa and triggers systemic inflammatory response, bacteremia and sepsis.
- Clinical manifestations: Extremely toxic, it can cause critical illness independently, presenting as persistent watery stool, mucohemorrhagic stool, severe abdominal pain accompanied by high fever, lethargy and dehydration. Advanced cases may suffer intestinal perforation and sepsis with a high mortality rate. When acting synergistically with Toxin A, their toxic effects are superimposed, leading to more severe mucosal injury.
- Other properties: More thermostable than Toxin A, it requires heating at 70°C for 10 minutes for inactivation. Resistant to degradation by intestinal proteases, it maintains toxicity for a long duration and boasts a high clinical detection rate, serving as the core biomarker for diagnosing Clostridioides difficile infection.
(III) Practical Comparison Table of Toxin A and Toxin B
Comparing the core characteristics of the two toxins enables rapid assessment of disease severity in pets and guides treatment strategies. The table below adopts practical descriptions without complicated academic jargon:
| Differentiation Item | Toxin A (Enterotoxin, TcdA) | Toxin B (Cytotoxin, TcdB) |
| Toxin Category | Enterotoxin, acts on intestinal mucosal surface | Cytotoxin, penetrates intestinal mucosal cells |
| Toxicity Level | Weak, 1/10–1/100 of Toxin B | Extremely potent, key virulence factor for severe infection |
| Main Pathogenic Effect | Destroys mucosal tight junctions, causes watery diarrhea and mucosal edema | Damages cytoskeleton, triggers cell necrosis and pseudomembrane formation |
| Clinical Signs | Predominantly mild cases: watery stool, slight abdominal pain, no systemic symptoms | Predominantly severe cases: mucohemorrhagic stool, high fever, risk of sepsis |
| Thermal Stability | Poor; inactivated after heating at 60℃ for 10 min | Good; inactivated after heating at 70℃ for 10 min |
| Clinical Detection Rate | Low; only detectable in mild or partial cases | High; detectable in all severe cases |
| Prognosis | Favorable, rare recurrence | Poor, high recurrence risk, high mortality in severe cases |
| Synergistic Effect | Coexistence leads to superimposed toxicity, aggravated mucosal injury and faster disease progression | Coexistence leads to superimposed toxicity, aggravated mucosal injury and faster disease progression |
III.Life Cycle and Epidemiological Transmission Trends
(I) Core Stages of the Life Cycle
The life cycle of Clostridioides difficile can be summarized as: spore colonization – proliferation – toxin production – excretion – spore transmission. No complex host switching occurs throughout the whole process, making it well-adapted to the intestinal tract of pets as well as daily breeding and veterinary clinical environments.
- Spore colonization: Spores enter the intestines of dogs and cats via the fecal-oral route. Resistant to gastric acid and aerobic intestinal segments, spores germinate into vegetative cells upon reaching the anaerobic distal small intestine and colon, then adhere to the surface of intestinal mucosal epithelial cells to complete colonization.
- Proliferation and toxin production: When intestinal dysbiosis arises (caused by antibiotic administration, stress, concurrent intestinal infection, etc.), beneficial flora decreases sharply. Vegetative cells multiply rapidly; once pathogenic strains reach a critical concentration, they secrete Toxin A and Toxin B, triggering intestinal inflammation and clinical signs.
- Excretion and sporulation: Vegetative cells and toxins are shed with feces after replication. Part of the vegetative cells transform into spores inside the gut or after excretion. Feces carry extremely high spore loads and serve as the primary source of infection.
- Transmission and re-colonization: Spores in feces contaminate feed, drinking water, pet supplies and the surrounding environment. Healthy pets ingest spores via the fecal-oral route after exposure, completing the transmission cycle. Asymptomatic carrier pets may experience renewed bacterial proliferation and toxin production under stress, leading to recurrent clinical episodes.
(II) Key Epidemiological Points
- Primary transmission route: Fecal-oral transmission predominates. Feces from infected or asymptomatic carrier pets contaminate pet supplies and the environment; healthy pets ingest spores upon contact and develop infection. Environmental transmission (spore-contaminated cages, equipment, staff clothing) and nosocomial transmission (inadequate disinfection of clinical instruments, inappropriate antibiotic use) are also prevalent.
- Susceptible animals: High-risk groups include pets on long-term antibiotic therapy, puppies and kittens aged 1–6 months, immunocompromised individuals (tumors, chronic enteropathy, etc.), strays, multi-pet household animals, and pets with recent stress exposure. Immunocompetent adult dogs and cats kept alone and fed cooked diets are mostly asymptomatic carriers and rarely develop overt clinical disease.
- Epidemiological characteristics: Infections occur year-round with slightly higher incidence in winter and early spring. The incubation period ranges from 2 to 10 days, and peak onset falls within 1–2 weeks during or after antibiotic treatment. Cases are mostly sporadic, but clustered outbreaks frequently break out in veterinary clinics, catteries and multi-pet households. The recurrence rate is high, and co-infections are common.
IV. Pathogenic Mechanism
The core pathogenesis of Clostridioides difficile relies on colonization induced by intestinal dysbiosis plus synergistic mucosal damage from Toxin A and Toxin B. The bacterium itself is non-invasive, and all clinical manifestations arise solely from the effects of the two toxins.
Triggering factors: Long-term administration of broad-spectrum antibiotics ranks as the most prevalent trigger, followed by stress, concurrent intestinal infection, malnutrition and other conditions. These factors drastically reduce beneficial gut flora and disrupt intestinal homeostasis. The resulting anaerobic microenvironment facilitates spore germination and vegetative cell proliferation.
Synergistic toxic injury: After virulent strains multiply, they secrete both toxins. Toxin A first disrupts tight junctions of the intestinal mucosa, inducing watery diarrhea and mucosal edema, which creates entry opportunities for Toxin B. Once Toxin B invades mucosal epithelial cells, it destroys the cytoskeleton and causes cellular necrosis and pseudomembrane formation. In severe cases, toxins penetrate damaged mucosa into the bloodstream, triggering systemic inflammatory response and multi-organ lesions.
Disease exacerbation: Damaged intestinal lining loses its barrier function, further accelerating the proliferation and toxin production of C. difficile, forming a vicious cycle: mucosal injury → increased toxin secretion → aggravated tissue damage. Concurrent infection with other enteric bacteria intensifies inflammation and diarrhea, prolonging the recovery period.
V. Clinical Signs in Dogs and Cats
Clinical manifestations of Clostridioides difficile infection are closely associated with toxin type, pet age and immune status. Intestinal dysfunction serves as the core presentation, with slight discrepancies between dogs and cats. Cases are mainly categorized into mild infection, severe infection, chronic infection and subclinical carriage.
(I) Clinical Signs in Dogs
Mild infection (single Toxin A infection / activated subclinical carriage): Watery or pasty yellowish-white to pale yellow-green stool with a small amount of mucus, no blood; defecation 3–6 times daily with strong fetid odor. Mild abdominal discomfort is present, while mentality and appetite remain nearly normal with absent or low-grade fever. Symptoms resolve rapidly with timely intervention.
Severe infection (combined Toxin A & B infection / isolated Toxin B infection): Persistent watery diarrhea occurring 6–10 times daily, stool loaded with massive mucus, streaks or clots of blood; white pseudomembranes may be observed in some samples. Signs include severe abdominal pain, frequent vomiting, high fever (39.5–40.5°C), lethargy, anorexia and rapid dehydration. Severe complications such as pseudomembranous enteritis, intestinal perforation and bacteremia may develop, with a mortality rate of 25%–35%.
Chronic infection / recurrent episodes: Recurrent alternating loose and formed stool, accompanied by mild inappetence and weight loss lasting several weeks. Flare-ups are easily triggered by stress or short courses of antibiotics.
(II) Clinical Signs in Cats
Mild infection: Predominantly pasty stool with occasional watery consistency and minimal mucus, no blood; defecation 2–4 times daily with mild odor. Vomiting rarely occurs, cats maintain normal activity and appetite without fever. Cats exhibit higher tolerance to Toxin A, so mild cases are often overlooked.
Severe infection: Unremitting watery, mucohemorrhagic stool with visible pseudomembranes in some cases, defecation 4–8 times daily; severe cases present anal atony and fecal incontinence. Associated signs include mild vomiting, abdominal pain, moderate fever (38.8–39.8°C), lethargy, anorexia and dehydration. Kittens are prone to hypoglycemia. Severe cases may progress to bacteremia and hepatic/renal injury, carrying a mortality rate of 15%–25%, lower than that in dogs.
Subclinical carriage: Adult cats have a higher asymptomatic carriage rate than dogs. No clinical signs appear, yet spores are continuously shed in feces, turning carriers into infection sources. Overt disease can emerge under long-term antibiotic administration or stress.
VI. Standardized Treatment Protocols
The core treatment strategy for Clostridioides difficile infection consists of eliminating predisposing factors, standardized anti-infective therapy, symptomatic supportive care and intestinal flora restoration. Regimens should be tailored according to toxin type and disease severity, with the mandatory preliminary step of discontinuing precipitating antibiotics. Below are standardized clinical treatment principles and tiered protocols.
(I) General Treatment Principles
- Immediately withdraw broad-spectrum antibiotics that triggered infection, and eliminate stress, environmental contamination and other predisposing factors.
- Prioritize correction of dehydration and electrolyte imbalance, plus intestinal mucosal protection.
- Administer targeted susceptible antibiotics only for clinical symptomatic or severe cases.
- Modulate gut microbiota and repair intestinal barrier function.
- Prevent complications; implement full isolation to block transmission.
(II) Tiered Treatment Protocols
Mild Cases (Toxin A only, alert mental status, mild diarrhea, slight dehydration)
- Eliminate triggers: Discontinue broad-spectrum antibiotics; raise the pet in separate isolation; switch to highly digestible intestinal prescription diet; withhold raw meat and table scraps.
- Supportive care: Oral veterinary oral rehydration salts administered in small frequent doses; smectite powder for mucosal protection combined with veterinary-specific probiotics to restore gut flora.
- Optional anti-infective therapy: If diarrhea persists over 48 hours, oral metronidazole (dogs: 10–15 mg/kg, cats: 5–10 mg/kg) twice daily for 5–7 consecutive days.
- Prognosis: Most patients recover within 5–7 days with low recurrence; follow-up toxin testing is unnecessary.
Severe Cases (Toxin A+B co-infection / Toxin B mono-infection, mucohemorrhagic stool, hyperthermia, moderate dehydration)
- Eliminate triggers: Discontinue all broad-spectrum antibiotics; strict isolation; house in a quiet warm environment at 25–28 °C; withhold food for 24 hours to reduce gastrointestinal load, only offer rehydration solution or plain water.
- Supportive care: Subcutaneous fluid therapy for moderate dehydration; immediate intravenous fluid resuscitation for severe dehydration to correct acidosis and hypokalemia. Maropitant injection for anti-emesis; smectite plus kaolin-pectin complex to control diarrhea. Subcutaneous B-complex vitamins to facilitate mucosal repair; nutritional paste or nasogastric feeding for anorexic juveniles; bupleurum injection intramuscularly to reduce fever in febrile patients.
- Mandatory anti-infective therapy: First-line metronidazole (dogs: 15–20 mg/kg, cats: 10–15 mg/kg), oral or intravenous administration twice daily for 7–10 days. Avoid excessive dosages in cats to prevent neurotoxicity. Switch to oral vancomycin for metronidazole-resistant strains; veterinary immunoglobulin may be supplemented to boost immunity for critical patients.
- Prognosis: Recovery typically takes 7–10 days. Toxin B-positive cases carry high recurrence risk; intestinal conditioning should continue for another 1–2 weeks after clinical resolution.
Critical Cases (Pseudomembranous enteritis, bacteremia, severe dehydration, somnolence)
- Emergency intervention: Intravenous fluid resuscitation for shock; hydroxyethyl starch infusion to expand blood volume; continuous vital sign monitoring, oxygen supplementation if required.
- Anti-infective therapy: Combined vancomycin + metronidazole for an extended 10–14 day course. Adjust antibiotics based on antimicrobial susceptibility testing if blood cultures return positive.
- Symptomatic management: Hepatoprotective and nephroprotective agents; prophylaxis against intestinal perforation and peritonitis; intensive nursing care including perianal cleaning and regular turning.
- Prognosis: High mortality rate (25%–35%); full inpatient monitoring is required. Post-recovery follow-up includes fecal toxin assay and complete blood count.
Recurrent Cases
Alternate metronidazole and vancomycin for a total 14-day course; long-term probiotic supplementation for 1–2 months alongside intestinal prescription diet. Avoid repeated broad-spectrum antibiotic use and stress stimuli. Conduct fecal toxin testing 3–7 days post discharge; discontinue antibiotics only after two consecutive negative toxin results.
VI. Protocolos de tratamiento estandarizados
El eje terapéutico de la infección por Clostridioides difficile es la eliminación de factores predisponentes, terapia antiinfecciosa reglada, soporte sintomático y restauración de la microbiota intestinal. Los tratamientos se adaptan al tipo de toxina y gravedad del cuadro, siendo condición indispensable suspender previamente los antibióticos causantes. A continuación se detallan los principios terapéuticos clínicos y protocolos escalonados.
(I) Principios generales de tratamiento
- Suspender inmediatamente los antibióticos de amplio espectro que provocaron la infección y eliminar estrés, contaminación ambiental y otros factores desencadenantes.
- Corregir prioritariamente la deshidratación y desequilibrios electrolíticos, además de proteger la mucosa intestinal.
- Administrar antibióticos sensibles dirigidos solo en casos sintomáticos o graves.
- Regular la microbiota intestinal y reparar la barrera mucosa digestiva.
- Prevenir complicaciones y mantener aislamiento total para interrumpir la transmisión.
(II) Protocolos escalonados de tratamiento
Casos leves (solo toxina A, animal alerta, diarrea leve, ligera deshidratación)
- Eliminación de factores predisponentes: suspender antibióticos de amplio espectro, alojar la mascota en aislamiento individual, cambiar a dieta prescrita digestible, retirar carne cruda y restos de comida humana.
- Soporte sintomático: sales de rehidratación oral veterinarias administradas en dosis pequeñas y frecuentes; polvo de montmorillonita para protección mucosa combinado con probióticos específicos para mascotas que restauran la flora intestinal.
- Terapia antiinfecciosa opcional: si la diarrea persiste más de 48 horas, metronidazol oral (perros: 10–15 mg/kg, gatos: 5–10 mg/kg) dos veces al día durante 5 a 7 días consecutivos.
- Pronóstico: la mayoría se recupera en 5–7 días con baja recurrencia, no es necesario repetir análisis de toxinas.
Casos graves (coinfección toxina A+B / infección exclusiva toxina B, heces mucosanguinolentas, fiebre alta, deshidratación moderada)
- Eliminación de factores predisponentes: suspender todos los antibióticos de amplio espectro, aislamiento estricto, alojamiento en entorno tranquilo y cálido (25–28 °C), ayuno de 24 horas para reducir la carga gastrointestinal, solo se ofrece suero rehidratante o agua simple.
- Soporte sintomático: sueroterapia subcutánea en deshidratación moderada; sueroterapia intravenosa inmediata en deshidratación grave para corregir acidosis e hipopotasemia. Inyección de maropitant para controlar vómitos; montmorillonita junto a complejo caolín-pectina para frenar la diarrea. Vitaminas del complejo B por vía subcutánea para reparar la mucosa; pasta nutricional o sonda nasogástrica en cachorros/gatitos que rechacen el alimento; inyección de bupleurum intramuscular para bajar la fiebre.
- Terapia antiinfecciosa obligatoria: metronidazol de primera elección (perros: 15–20 mg/kg, gatos: 10–15 mg/kg), vía oral o intravenosa dos veces al día durante 7–10 días. Evitar dosis elevadas en gatos para prevenir neurotoxicidad. En cepas resistentes a metronidazol se cambia a vancomicina oral; se puede añadir inmunoglobulina veterinaria para reforzar la respuesta inmune en pacientes graves.
- Pronóstico: la recuperación suele durar 7–10 días. Los casos positivos para toxina B tienen alto riesgo de recaída; se debe continuar la recuperación intestinal durante 1–2 semanas tras la desaparición de signos.
Casos críticos (enteritis pseudomembranosa, bacteriemia, deshidratación severa, somnolencia)
- Intervención de urgencia: sueroterapia intravenosa para revertir shock, infusión de almidón hidroxietílico para expandir volumen sanguíneo, monitorización continua de signos vitales y oxigenoterapia si es preciso.
- Terapia antiinfecciosa: asociación vancomicina + metronidazol con duración extendida de 10–14 días. Modificar el tratamiento según antibiograma si el hemocultivo resulta positivo.
- Manejo sintomático: agentes hepatoprotectores y nefroprotectores, profilaxis contra perforación intestinal y peritonitis, cuidados intensivos con limpieza perianal y cambios de postura periódicos.
- Pronóstico: alta tasa de mortalidad (25%–35%); requiere hospitalización y monitorización constante. Tras recuperación se debe realizar análisis de toxinas fecales y hemograma de control.
Casos recurrentes
Alternar metronidazol y vancomicina durante 14 días en total; suplementación prolongada con probióticos durante 1–2 meses junto a dieta intestinal prescrita. Evitar el uso repetido de antibióticos de amplio espectro y situaciones generadoras de estrés. Realizar análisis de toxinas en heces entre 3 y 7 días tras el alta; suspender antibióticos solo tras dos resultados negativos consecutivos.
VII. Prevention, Control & Precautions (Top Priority)
The core of prevention and control against Clostridioides difficile infection lies in thorough environmental disinfection and strict isolated care, alongside adequate zoonotic protection. Key measures are listed below:
(I) Daily Prevention & Control Measures
- Environmental disinfection Wipe pet supplies, floors and cages daily with diluted chlorine-based disinfectant (1:100) or peracetic acid, leave for 10–15 minutes then rinse with clean water. Veterinary instruments must be autoclaved or soaked in chlorine disinfectant for 30 minutes. Seal and discard infected pets’ feces, and disinfect contaminated areas immediately. Ventilate premises 2–3 times per day to reduce spore concentration.
- Isolated nursing Separate infected pets right away; maintain isolation for an additional 7 days after fecal toxin tests turn negative. Use dedicated tools only for isolated patients. Wash hands thoroughly with soap and running water or sanitize with chlorine disinfectant after handling infected animals.
- Rational antibiotic administration Prescribe antibiotics only when clinically indicated to avoid overuse of broad-spectrum agents. Perform bacterial culture and antimicrobial susceptibility testing prior to antibiotic therapy whenever possible. Supplement probiotics for pets on long-term antibiotic courses.
- Feeding & husbandry management Feed fresh, easily digestible cooked diets; withhold raw meat, table scraps and spoiled feed. Provide boiled drinking water instead of raw tap water. Conduct regular deworming and core vaccination. Reduce stocking density in multi-pet households and assign separate supplies for each animal.
- Quarantine for new arrivals Quarantine new pets (especially strays and newly purchased animals) for a minimum of 2 weeks. Monitor stool consistency and perform toxin testing if needed; introduce to resident pets only after confirming negative results.
(II) Zoonotic Protection Guidelines
Clostridioides difficile is a zoonotic pathogen. The elderly, children, pregnant women and immunocompromised individuals face higher risks of severe illness. Pet owners shall follow these protective rules:
- Wear disposable gloves when handling infected pets or cleaning feces. Wash hands with soap and running water afterward, or disinfect with chlorine solution / 75% ethanol.
- High-risk groups shall minimize direct contact with infected pets and their feces; ask other caregivers to assist if necessary. Avoid sharing beds or close physical contact with sick animals.
- Disinfect the pet’s living space daily. Dispose of bedding and towels as single-use items, or boil them thoroughly then sun-dry for reuse.
- If owners develop diarrhea, abdominal pain or fever after exposure (especially during or after antibiotic treatment), seek prompt medical attention and inform physicians of contact with a C. difficile-infected pet.
Summary
Clostridioides difficile is a common opportunistic pathogenic anaerobic bacterium in the intestinal tract of pets. Its core harm stems from the synergistic damage caused by Toxin A and Toxin B. Antibiotic overuse and stress are the main predisposing factors. The strong resistance of its spores increases the difficulty of transmission prevention and control. As a zoonotic pathogen, it requires rigorous vigilance.
Pet owners should standardize daily feeding and management, avoid antibiotic abuse, and maintain thorough environmental disinfection. If pets develop diarrhea, especially worsening gastrointestinal symptoms after antibiotic treatment, prompt medical examination for Clostridioides difficile infection is required, with treatment and nursing conducted in strict accordance with veterinary advice.
Scientific intervention and precise prevention and control can effectively protect pet health and reduce the risk of human infection.