The Culprit Behind the Respiratory Infection Outbreak
01 Causes of the Outbreak
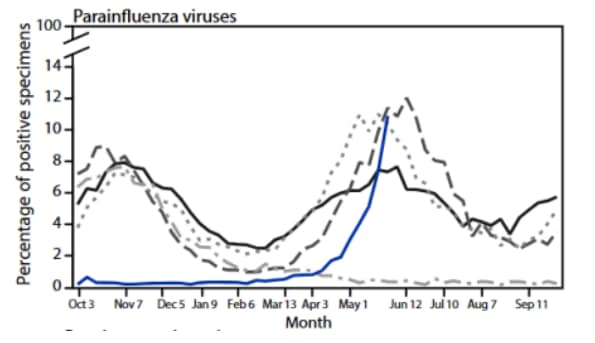
In 2021, researchers from the U.S. Centers for Disease Control and Prevention (CDC) published a study analyzing trends in influenza and other respiratory viruses since the onset of COVID-19 (2020–2021). The study found that between January 4 and April 4, 2020, the weekly percentage of RSV-positive cases dropped from 15.3% to 1.4% — a decline of more than 50% compared with the same period in the previous four years — and remained at historic lows (weekly <1.0%) the following year. In contrast, during the four preceding years, the weekly percentage of RSV-positive cases had exceeded 3.0% starting in October, with peaks ranging from 12.5% to 16.7% in late December. Substantial reductions were also observed in the weekly positivity rates of other respiratory viruses.
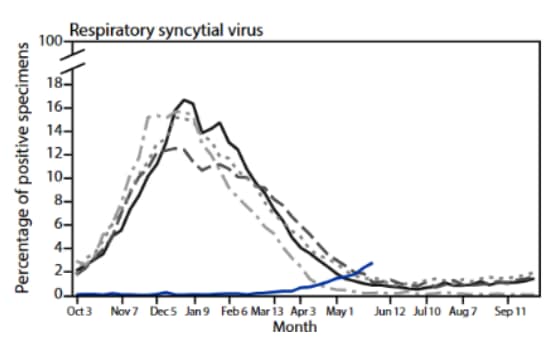
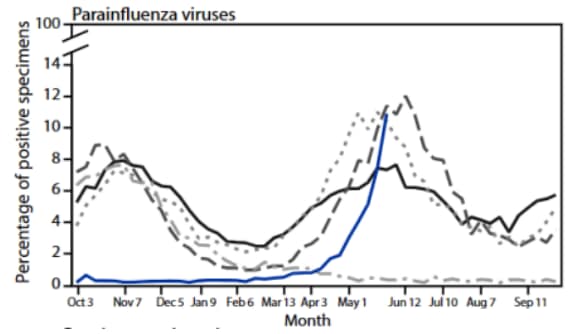

Percentage of respiratory syncytial virus (RSV), common human coronaviruses, and parainfluenza virus positive samples by month in the United States, 2016–2021
Source: MMWR
Looking at the timeline, the COVID-19 pandemic in the United States began in early 2020, when the U.S. government implemented strict epidemic control measures and the public was instructed to stay at home in isolation. As the pandemic progressed, restrictions were gradually lifted, and in April 2021, domestic travel was reopened for fully vaccinated individuals.
At this point, as can be observed from the data, the positivity rates of these respiratory viruses began to rise starting in April 2021, and their regular epidemic cycles gradually resumed.
However, there was one exception: recombinant adenoviruses returned to their normal circulation much more quickly. Due to their non-enveloped structure, adenoviruses can survive longer in the external environment, and their transmission is less affected by non-pharmaceutical interventions. As a result, their positivity rates declined to a smaller extent compared with other enveloped respiratory viruses, and they recovered at a faster pace.

Percentage of respiratory adenovirus-positive samples by month in the United States, 2016–2021
Source: MMWR
Based on this, researchers predicted that the strict epidemic prevention measures implemented by governments during the COVID-19 pandemic reduced exposure opportunities for these respiratory viruses. Prolonged absence of natural infection also led to declining antibody levels against these viruses, creating an immunity gap. As a result, once control measures were lifted, a surge in respiratory virus infections was expected.
In the context of China’s prevention policies, COVID-19 was officially reclassified as a Class B infectious disease under Class B management in January 2023, marking the start of full reopening. As early as April to May of the same year, respiratory syncytial virus (RSV) already began to show an off-season small-scale outbreak. With winter being the typical RSV epidemic season, its increased transmissibility naturally led to a large-scale epidemic.
02 Etiology
Next, we will briefly introduce the RSV virus. RSV is a pneumovirus in the family Paramyxoviridae, first isolated from the respiratory tract of chimpanzees in 1956. It has two subtypes: A and B.During cell culture, RSV aggregates and buds through membrane raft bridging, causing fusion of adjacent cells and forming characteristic syncytia. The virus proliferates in the cytoplasm, where cytoplasmic inclusion bodies can be observed. It is named respiratory syncytial virus because its cytopathic effect forms syncytium-like structures.
Its pathological mechanism is quite interesting. There is a receptor in our body called nucleolin (NCL), which acts as an accomplice during RSV infection. RSV binds to insulin-like growth factor receptor 1 and protein kinase C, which generate intracellular signaling and recruit nucleolin to the cell surface where the virus is located. The virus then binds to nucleolin and enters the cell interior.

Structure of RSV
Source: Expert Consensus on the Diagnosis, Treatment and Prevention of Respiratory Syncytial Virus Infection in Children
03 Transmission Routes
Mainly transmitted through respiratory droplets and close contact. It is highly contagious, with an incubation period of 2–8 days.
04 Epidemiology
A 2015 study by the Global RSV Surveillance Network showed there were approximately 33.1 million new cases of RSV-associated acute lower respiratory tract infection (ALRTI) in children under 5 years old worldwide. Among them, 3.2 million children required hospitalization (accounting for 28% of all ALRTI cases), and 59,600 hospitalized children died (representing 13%–22% of ALRTI deaths). Ninety-nine percent of these deaths occurred in developing countries.
05 Clinical Manifestations
Symptoms are similar to influenza but also include more severe complications such as fever, cough, chest pain, wheezing, and dyspnea.Infections are more severe in infants and young children. Early manifestations include high fever, rhinitis, and pharyngitis, which later progress to bronchiolitis and pneumonia. Bronchiolitis can be classified as mild, moderate, or severe.
Severity Grading for RSV Bronchiolitis
| Item | Mild | Moderate | Severe |
| Oral intake | Normal | Decreased to half of normal | Decreased to more than half of normal or refusal to feed |
| Respiratory rate | Normal or slightly elevated | >60 breaths/min | >70 breaths/min |
| Retractions | None | Intercostal retractions, moderate | Marked intercostal retractions |
| Nasal flaring or grunting | None | None | Present |
| Oxygen saturation | >92% | 88%–92% | <88% |
| Mental status | Normal | Mild or intermittent irritability | Severe restlessness, lethargy |
06 Diagnosis
Virus isolation is the gold standard, but it is time consuming and labor intensive, making it unsuitable for routine clinical use.Second generation rapid antigen detection and PCR testing are more commonly applied. Antigen testing is less sensitive than nucleic acid testing, but results can generally be obtained within 30 minutes.Given the increasing prevalence of mixed infections, microfluidic multiplex nucleic acid respiratory panel testing represents a better choice. For more information on this, you may follow the WeChat official account “Chenghui Medical Technology”.
07 Treatment
The disease is somewhat self limiting, and supportive care is the mainstay of management.Oxygen therapy is indicated when oxygen saturation remains below 90%–92%.Pharmacological treatment may be used based on clinical conditions, including interferon, bronchodilators, corticosteroids, and hypertonic saline nebulization.Specific usage should follow the recommendations of a clinician.
08 Prevention
For enveloped viruses, personal protective measures are the most effective, such as frequent handwashing, mask wearing, and keeping warm during seasonal transitions.No related vaccine is currently available in China, but vaccine development is already underway and is expected to be launched soon.
Lastly, wish you all good health and smooth work. We also hope you will continue to follow Gangzhu Medical.
References:
Olsen, Sonja J et al. “Changes in Influenza and Other Respiratory Virus Activity During the COVID-19 Pandemic – United States, 2020–2021.” MMWR. Morbidity and Mortality Weekly Report, vol. 70, 29, 1013–1019, 23 Jul. 2021, doi:10.15585/mmwr.mm7029a1.
Drysdale, et al. Priorities for developing respiratory syncytial virus vaccines in different target populations. Sci. Transl. Med., 2020.
Expert Consensus on the Diagnosis, Treatment and Prevention of Respiratory Syncytial Virus Infection in Children.